For people who are at high risk for lung cancer— particularly individuals with a longtime smoking history—annual screenings are essential. Radiologists conduct these screenings by using a low-dose CT scan to get a detailed image of the lungs.
But these screenings sometimes reveal more than just lung health.
“The negative effects of smoking extend beyond just lung cancer,” says Tina Tailor, MD, Assistant Professor of Radiology in the Duke School of Medicine. “Cardiovascular disease is actually the leading cause of death in patients screened for lung cancer.”
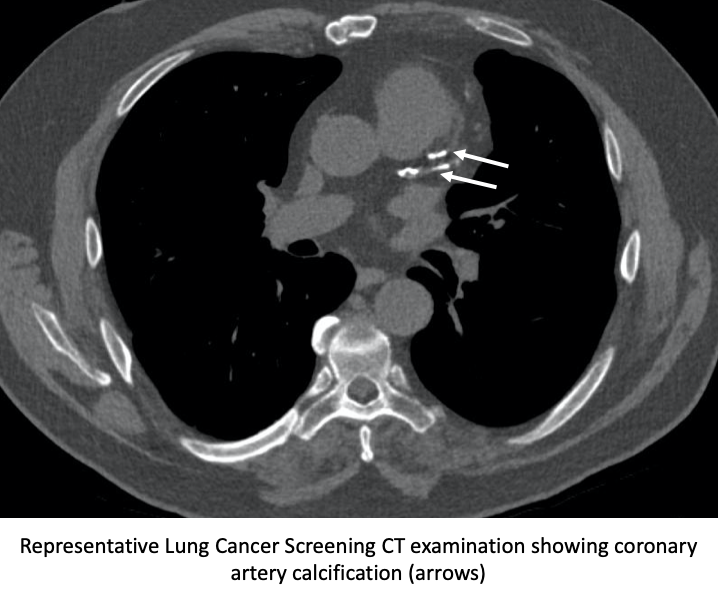
Coronary artery calcification (CAC), which is the build-up of calcium on the heart’s arteries, is visible on a CT scan, and is a known predictor of cardiovascular disease. It’s not unusual to find CAC in the lung cancer screening group—many people are at risk for both.
Statins, a class of drugs that lower cholesterol levels, are a common therapy used to prevent serious adverse cardiovascular events down the road. The American Heart Association has certain clinical criteria to determine if a patient should be on a statin.
However, a collaborative study led by Tailor and colleagues at UNC-Chapel Hill and Wake Forest University has found that most lung cancer screening patients who are statin eligible are not on a statin at the time of their screening. They also found that if CAC was reported by the radiologist, those patients were more likely to be prescribed a statin later on.
From reporting to prevention
“Lung cancer screening is a relatively new recommendation,” says Tailor, who acted as the co-principal investigator on the study. She was joined by co-PIs Caroline Chiles, MD, of Wake Forest Baptist Hospital, and Louise Henderson, PhD, of UNC-Chapel Hill.
“Through lung cancer screening, we may be able to look for markers of cardiovascular disease, and CAC is one of these.”
Tailor and her collaborators studied a cohort of over 5,000 lung cancer screening patients, finding that the vast majority of them met the criteria for preventative statin therapy. At the same time, most of those patients were not prescribed a statin when they came in for their screening exam.
“The knowledge gap that we were interested in here is, ‘How does the reporting of CAC at a screening exam affect downstream preventative statin therapy?’” she explains.
If the radiologist reported CAC, the study found that that the patient was more likely to be prescribed a statin afterward—a link that had not before been robustly established. The team plans to share the details of these findings in forthcoming publications and presentations.
The power of data
To make this data-heavy, multi-site collaboration work, the team relied on funding and data from the Carolinas Collaborative and project management from Duke CTSI Accelerator.
“CTSI provided us with an ideal opportunity for this group of researchers to bring in three clinical sites [Duke, UNC, and Wake Forest] with a high volume of lung cancer screening,” says Tailor. “It was the first time I had collaborated in this way.”
Tailor worked directly with Lisa Davis, MSPH, PhD, Director of Special Projects at Duke CTSI, and Janis Curtis, Associate Director of Duke’s Clinical Data Research Networks (CDRN) program. Data teams at all three sites extracted massive amounts of electronic health record (EHR) data from the Carolinas Collaborative datamart, creating datasets that were securely and effectively shared across institutions.
“Dr. Tailor’s collaborative study is a great example of how the CDRNs in which Duke participates can support clinical research,” says Curtis. “The availability of large amounts of coded EHR data in an electronic format makes it significantly easier to work with very large numbers of patient records.”
Davis, in her role as Project Leader with Duke CTSI Accelerator, provided project management, helping the team complete their study across a one-year timeline despite the complexities of having multiple sites.
“Project leadership and connections to resources can really go a long way in helping study teams advance important research,” Davis says. “It was truly an honor to work with Dr. Tailor and team to help move the work forward efficiently.”
The collaborative nature of the project was essential, according to Tailor. “With a study like this that is retrospective, the ability to have data from multiple centers gave us more statistical power to answer our questions.”
Armed with their new findings, the multi-institutional team will explore ways to improve the guidelines for lung cancer screening, and work toward developing recommendations for radiologists to report CAC in a standardized manner.
“We’ve shown that when we do report these findings, they lead to changes downstream,” Tailor says—changes that could help prevent adverse cardiovascular events for patients.
For more information about translational funding and project management, visit CTSI Accelerator.
For more information about using Clinical Data Research Networks to conduct multi-site research using well-curated EHR, visit the CDRN Program.
Duke CTSI is supported in part by the Duke CTSA grant #UL1TR002553.